Association of Moderate Hypothermia at Admission with Short-Term and Long-Term Outcomes in Extremely Low Birth Weight Infants
Article information

Abstract
Purpose
Extremely low birth weight (ELBW) infants exhibit immature thermoregulation and are easily exposed to hypothermia. We investigated the association between hypothermia on admission with short- and long-term outcomes.
Methods
Medical records of ELBW infants admitted to the neonatal intensive care unit of a tertiary medical center between June 2012 and February 2017 were retrospectively analyzed. Upon admission, the axillary body temperature was measured. Moderate hypothermia was defined as admission temperature below 36 ℃.
Results
A total of 208 infants with gestational age of 26.4±2.3 weeks and birth weight of 746.7±154.9 g were included. Admission temperature ranged from 33.5 to 36.8 ℃ (median 36.1 ℃). Univariate analyses of maternal and infant characteristics were performed for moderately hypothermic and control (normothermic to mildly hypothermic) infants. Lower gestational age, lower birth weight, and vaginal delivery correlated with moderate hypothermia. Logistic regression analyses adjusted for confounders revealed that the incidence of hemodynamically significant patent ductus arteriosus (hsPDA) was associated with moderate hypothermia in ELBW infants. Moreover, abnormal mental developmental index scores on the Bayley Scales of Infant Development II at a corrected age of 18 to 24 months were associated with moderate hypothermia, but not with the psychomotor developmental index, incidence of blindness, deafness, or cerebral palsy.
Conclusion
Moderate hypothermia at admission is not only correlated with short-term neonatal morbidities such as hsPDA, but may also be associated with long-term neurodevelopmental impairment in ELBW infants. Future large-scale studies are required to clarify the long-term consequences of hypothermia upon admission.
INTRODUCTION
Neonatal infants lose heat immediately after birth through mechanisms such as radiation, convection, evaporation, and conduction [1,2]. Preterm infants are more vulnerable to reduced temperatures because of their higher ratio of skin surface area to weight, highly permeable skin, decreased subcutaneous fat, and less-developed stores of brown fat [3,4]. The association between admission temperature and neonatal mortality and morbidity in preterm infants has been studied using data from multiple centers [5-9]. However, despite large sample sizes, such studies are often biased when investigating outcomes because of differences in neonatal care and temperature management among centers. Moreover, it is unclear whether a low temperature at admission is only associated with short-term outcomes, or if it influences long-term outcomes. This study aimed to investigate whether low admission temperatures in extremely low birth weight (ELBW) infants are associated with short- and long-term outcomes.
MATERIALS AND METHODS
1. Study population
ELBW infants weighing 400 to 999 g treated in the neonatal intensive care unit (NICU) at a tertiary medical center between June 2012 and February 2017 were selected. Infants born at another center or with major congenital anomalies were excluded from the study. Demographic and clinical data were retrospectively collected from medical records after obtaining approval from the Institutional Review Board of the tertiary medical center.
2. Temperature management and measurement methods
The temperature in the delivery room was maintained between 24 and 26 °C. An infant radiant warmer and cap were applied to all newborns [10]. A polyethylene plastic bag was used for infants with a birth weight of less than 1,000 g [11]. The infant’s admission temperature was recorded immediately after entering the NICU. An electronic thermometer, MT200 (Microlife, ONBO Electronic [Shenzhen] Co. Ltd.) axillary temperature was measured at admission. Moderate hypothermia, mild hypothermia, and normothermia were defined as admission temperature of 32.0–35.9, 36.0–36.4, and 36.5–37.5 °C, respectively, according to the World Health Organization classification [12]. Regarding the median admission temperature of 36.1 °C, outcome variables of the moderate hypothermia group and normothermia to mild hyperthermia group were compared to assess the association of hypothermia and clinical outcomes.
3. Outcome variables
Short-term outcome variables included mortality and neonatal morbidity. Mortality was defined as death prior to discharge. Hemodynamically significant patent ductus arteriosus (hsPDA) was defined as PDA requiring medical or surgical treatment. Bronchopulmonary dysplasia (BPD) was classified according to the 2001 National Institute of Child Health and Human Development criteria. The incidences of moderate-to-severe BPD, grade III or IV intraventricular hemorrhage (IVH), and necrotizing enterocolitis (NEC) were analyzed. The IVH grading was determined according to Papile’s classification. NEC was assessed using a modified Bell staging system. Early onset sepsis was defined as culture-proven bacterial sepsis occurring within 72 hours of birth. Long-term neurodevelopmental outcomes were assessed at a corrected age of 18 to 24 months. The Bayley Scales of Infant Development II test and incidence of blindness, deafness, and cerebral palsy were used to evaluate neurodevelopmental impairments. A mental developmental index (MDI) <70 or psychomotor developmental index (PDI) <70 was considered abnormal.
4. Statistical analysis
Data were analyzed using SPSS software version 21.0 (SPSS Inc.). Categorical variables were analyzed using the chi-square and Fisher’s exact tests. Continuous variables were analyzed using Student’s t-test and the Mann-Whitney U-test. Associations between moderate hypothermia and clinical outcomes were analyzed using univariate analysis. Logistic regression models were used to adjust for the confounding factors. A P-value less than 0.05 was considered statistically significant.
RESULTS
1. Infant characteristics
Of 230 eligible ELBW infants, 208 infants with a mean±standard deviation gestational age of 26.4±2.3 weeks and birth weight of 746.7±154.9 g were enrolled in the study. Two infants born at another center and 20 infants with major congenital anomalies were excluded. The median admission temperature was 36.1 °C with an interquartile range of 35.7 to 36.3 °C. Thirteen infants (0.6 %) showed normal admission temperature (36.5 to 37.5 °C), 128 infants (61.5%) showed mild hypothermia (36.0 to 36.4 °C), 67 infants (32.3%) showed moderate hypothermia (32.0 to 35.9 °C), and no infants showed severe hypothermia (below 32.0 °C).
2. Baseline maternal and neonatal characteristics
We performed univariate analysis between the moderate hypothermia and control groups (normothermia to mild hypothermia). The effect of maternal conditions, intrapartum variables, and infant characteristics were analyzed (Table 1). Infants in the moderate hypothermia group showed lower gestational age, birth weight, cesarean delivery rate, and Apgar score at 1 and 5 minutes. Parity, rate of multiple pregnancies, ruptured membranes, oligohydramnios, and use of antenatal corticosteroids did not differ between the two groups.

Baseline Maternal and Neonatal Characteristics
3. Short-term outcomes according to admission temperature
Table 2 shows a comparison of the mortality and early neonatal morbidities between the moderately hypothermic and control groups. The mortality rates did not differ between the two groups. In the univariate analysis, the incidence of respiratory distress syndrome (RDS) and hsPDA were associated with moderate hypothermia. After correcting for gestational age, birth weight, and delivery mode, only hsPDA levels were associated with moderate hypothermia. Other neonatal morbidities, such as severe IVH, NEC, early onset sepsis, and BPD, were not correlated with low admission temperatures.
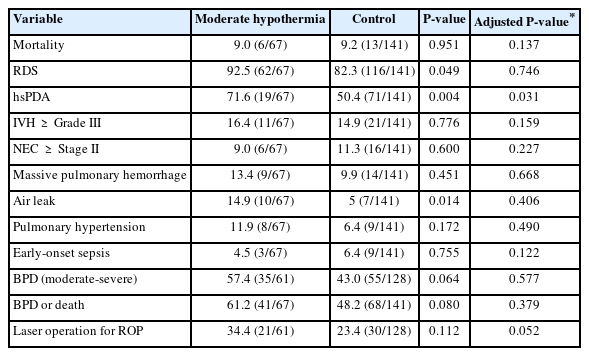
Association of Mortality and Early Neonatal Morbidities with Moderate Hypothermia
4. Long-term outcomes according to admission temperature
Table 3 shows a comparison of long-term outcomes between the moderate hypothermia and control groups. Of the 61 infants in the moderate hypothermia group, 49 were followed up with at a corrected age of 18 to 24 months. Of the 128 surviving infants in the control group, 113 were followed up with at a corrected age of 18 to 24 months. Follow-up rates were 80.3% and 88.3%, respectively. However, the Bayley Scales of Infant Development II tests were only performed in 36 and 76 patients, respectively. After adjusting for gestational age, birth weight, mode of delivery, and IVH, moderate hypothermia was associated with a MDI <70 on the BSID-II at a corrected age of 18 to 24 months. IVH was adjusted for in multivariate analysis, as it is associated with higher odds of moderate-to-severe neurodevelopmental impairment [13]. A PDI <70, blindness, deafness, and cerebral palsy were not associated with moderate hypothermia.

Association of Long-Term Outcomes with Moderate Hypothermia
DISCUSSION
This study investigated the association between short- and long-term outcomes and admission hypothermia in ELBW infants at a single center. ELBW infants with moderate hypothermia at admission were born at a younger gestational age with lower body weights and higher vaginal delivery rates. The incidence of hsPDA and the rate of BSID-II MDI <70 were associated with moderate hypothermia, indicating that hypothermia at admission may affect both short- and long-term outcomes in ELBW infants.
Previous multicenter studies have shown an association between admission temperature and mortality in preterm infants [5-8]. In addition, the Korean Neonatal Network study on very low birth weight infants consistently demonstrated that infants with lower admission temperatures had increased odds of mortality [14]. However, our data did not reveal any differences in mortality rates between the moderate hypothermia and control groups. This may be due to the small sample size and high overall survival. Short-term neonatal morbidities such as BPD, IVH, NEC, retinopathy of prematurity (ROP), and sepsis are associated with a low admission temperature [5,6,8]. In the present study, the incidence of hsPDA was higher in the moderate hypothermia group compared with the control. Other morbidities such as RDS, severe IVH, pulmonary hypertension, BPD, and ROP requiring surgery seemed to be more prevalent in moderately hypothermic infants, but the difference was not statistically significant. Hypothermia may negatively affect the smooth fetal-to-neonatal transition, resulting in increased respiratory distress and persistent pulmonary hypertension [5]. Hypothermia in newborn infants increases oxygen and energy consumption, metabolic acidosis, and hypoglycemia, which may lead to hemodynamic instability [15,16]. Postnatal ductal closure is facilitated by increased alveolar oxygen content [17]. The series of clinical conditions of admission hypothermia leading to hypoxia and hemodynamic instability may have contributed to the increased incidence of hsPDA in hypothermic infants.
To date, a small number of studies have investigated the correlation between admission temperature and long-term neurodevelopmental outcomes. According to a Canadian Neonatal Network study on extremely low-gestational-age neonates, hypothermic infants compared to normothermic infants showed increased odds of death or neurodevelopmental impairment at a corrected age of 18 to 21 months [18]. Another recent study demonstrated that a higher admission temperature was associated with a lower incidence of death and neurodevelopmental impairment at 3 years of age in VLBW infants [19]. In our study, hypothermic ELBW infants showed a higher prevalence of BSIDII MDI scores <70; however, due to follow-up losses and missed BSID-II examinations in relatively well-growing infants, the incidence of neurodevelopmental impairment in our study may not be accurate. The mechanisms underlying the adverse long-term outcomes associated with hypothermia remain unclear. Hypothermia in preterm infants increases neonatal morbidity. Neonatal morbidities, such as IVH, BPD, and NEC, are correlated with long-term neurodevelopmental impairment [20]. Prolonged hospital stays due to such morbidities may correlate with worse neurodevelopmental outcomes. Moreover, the medical or surgical treatment for patent ductus arteriosus is associated with increased odds of neurodevelopmental impairment and low MDI scores [21]. The increased incidence of hsPDA in hypothermic infants may have affected the long-term outcomes in this study.
Previous studies in developed countries have shown that 36% to 53% of preterm infants (<32 to 33 weeks born) show admission hypothermia [8,9]. According to the Korean Neonatal Network study, admission hypothermia occurs in 74.1% of VLBW and in preterm infants less than 33 weeks, which is greater than the rate seen in developed nations [14]. In this study, the proportion of moderate hypothermia was 25.7%, which is higher than the 11.9% to 22.3% reported in other studies [8,9]. Standard thermal care strategies, such as maintaining an adequate delivery room temperature and using plastic bags, radiant warmers, and preheated transport incubators, should be emphasized.
This study showed that ELBW infants with moderate hypothermia had higher vaginal delivery rates. In such cases, admission hypothermia may occur because the delivery is often unplanned. A recent report demonstrated higher survival rates in ELBW infants with cesarean births than in those with vaginal birth [22]. We speculate that admission hypothermia may have affected survival in this study.
This study had several limitations. First, it was a retrospective observational study with a small sample size. Second, the followup rate at the corrected age of 18 to 24 months was low, resulting in an even smaller sample size for assessing long-term outcomes. Third, BSID-II tests were not routinely performed in all patients. Lastly, axillary temperature measured at admission may be lower than rectal temperature, and thus may not fully represent core body temperature [23]. The main strength of this study is that it is the first in Korea to assess long-term neurodevelopmental outcomes associated with admission temperature.
In summary, this study demonstrated that moderate hypothermia was associated with an increased incidence of hsPDA and an increased rate of BSID-II MDI <70. Our study suggests that the effects of moderate hypothermia upon admission may persist after discharge. Therefore, adequate thermoregulation should be reinforced in ELBW infants.
Notes
Ethical statement
This study was approved by the Institutional Review Board at Asan Medical Center (2017-0712), and the need for written informed consent was waived by the board.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contributions
Conception or design: E.J.
Acquisition, analysis, or interpretation of data: S.H.K., J.H.H., B.S.L., E.J.
Drafting the work or revising: S.H.K., J.J., J.M.L., H.N.L., B.S.L., E.J.
Final approval of the manuscript: All authors read and approved the final manuscript.
Funding
None
Acknowledgements
None