Neurodevelopmental Outcomes of Very-Low-Birth-Weight Infants without Severe Brain Lesions and Impact of Postnatal Steroid Use: A Single-Center Korean Study
Article information

Abstract
Purpose
We used the Bayley Scales of Infant and Toddler Development (BSID)-III to analyze the incidence and risk factors of developmental delay in very-low-birth-weight infants without severe brain lesions. We further examined the correlation between the cumulative dexamethasone dose and developmental assessment results.
Methods
We retrospectively analyzed data of preterm infants (birth weight <1,500 g) admitted to our neonatal intensive care unit between January 2014 to December 2020. The BSID-III scores obtained between the corrected ages of 12 and 24 months and after 24 months were analyzed. Developmental delay was defined as a composite score of <85 for the cognition, language, and motor domains. Univariate and multivariate analyses of developmental delay risk factors and developmental changes from the first to second BSID-III were performed. Correlations between the accumulated dexamethasone dose used for bronchopulmonary dysplasia (BPD) and the first and second test scores were analyzed.
Results
Seventy-one and thirty-six infants completed the first and second tests, respectively. In both tests, developmental delay was most commonly observed in the language domain (26.8%, 47.2%). In multivariate analysis, mild BPD was identified as a developmental delay risk factor (P<0.05), whereas prenatal steroid use reduced the developmental delay risk (P<0.05). All domain scores were lower in the second test than in the first test. The cognition and language domain scores in the second test decreased with increasing cumulative dexamethasone doses.
Conclusion
Very-low-birth-weight infants typically experience language delay, which can persist as they age.
INTRODUCTION
The survival rate of very-low-birth-weight infants (VLBWIs) is increasing, while the incidence of major complications in such infants is decreasing in many countries owing to medical advances and the development of various drugs and respiratory assist devices [1,2]. One study that analyzed the survival trend among extremely preterm neonates in the United States over the last two decades reported survival rates of 80% and 90% for neonates born at 25 and 27 weeks, respectively. However, the survival rates for neonates discharged without major morbidities were only 20% and 50%, respectively, indicating that chronic complications remain a challenge to be overcome in preterm infants [2].
For preterm infants, the primary goal is survival and independent and autonomous living as adults. Severe brain lesions, which commonly include severe intraventricular hemorrhage (IVH) and periventricular leukomalacia (PVL) are major risk factors for poor development. Brain ultrasonography and, if needed, brain magnetic resonance imaging (MRI) can be used to detect severe brain lesions during hospitalization. An imaging study reported that preterm infants without severe brain lesions can still experience severe developmental delay [3]. Bronchopulmonary dysplasia (BPD), which increases in incidence as the number of weeks of survival of preterm infants decreases, affects neurodevelopmental outcomes [4]. Currently, no treatment is available for this chronic disease. Postnatal steroids were actively used to wean infants off ventilator support until the mid-1990s [2]; however, they have only been used as a last resort since the report of cerebral palsy (CP) as a long-term complication of postnatal steroid use. Currently, postnatal steroids are used for a short period, not too early after birth, in infants with unfavorable conditions [5]. Normal development is necessary for VLBWIs, who are at a high risk of developing BPD, to enjoy a good quality of life as they grow older; however, this cannot be guaranteed owing to the limitations of the available treatments.
Imaging to examine severe brain lesions is often performed as a screening procedure, and developmental follow-up of individual infants after discharge is necessary. The Bayley Scales of Infant and Toddler Development (BSID) is one of the most widely used developmental assessment tools. The BSID-III assesses development across five domains (cognition, receptive language, expressive language, gross motor, and fine motor), in greater detail than does the BSID-II [6]. It evaluates whether infants are developing at a rate appropriate for their corrected age in months, and the scores determine whether such infants require rehabilitative therapy. The Korean Neonatal Network (KNN) recommends completing the BSID-III test between the corrected ages of 18 and 24 months; and at 3 years. In reality, most infants are lost to follow-up after discharge; as a result, few studies have been conducted on the development of VLBWIs.
Understanding the developmental state of preterm infants is important to ensure not only survival, but also a good quality of life. This study used BSID-III scores to analyze the incidence and risk factors of developmental delay and developmental changes observed in VLBWIs without severe brain lesions who were discharged from a single institution during a 7-year period. Additionally, this study investigated whether the cumulative dexamethasone dose and developmental assessment results were correlated with each other.
MATERIALS AND METHODS
1. Study population
Data collected from preterm infants with a birth weight of <1,500 g who were admitted to the neonatal intensive care unit (NICU) of our institution between January 2014 and December 2020 were retrospectively analyzed. Infants who completed the BSID-III test at the corrected age of 12 months after discharge were selected. Those with severe brain lesions, defined as IVH of grade III or higher, PVL, or brain deformities detected on ultrasonography or brain MRI, were excluded.
2. Study design
The BSID-III scores obtained between the corrected ages of 12 and 24 months and after 24 months were analyzed to examine development at the corrected ages of 1 and 2 years, respectively. Developmental delay was defined by a composite score of <85 on each of the following domains: cognition, language, and motor [7]; It was deemed severe when the composite score for each domain was ≤69. The language composite scores consist of a combination of expressive and receptive language subscales, while the motor composite scores consist of gross and fine motor subscales. Univariate and multivariate analyses were conducted to determine the risk factors for developmental delay. Additionally, the developmental changes observed in infants who completed both BSID-III tests were examined.
To investigate the effect of dexamethasone use on BPD development, we analyzed the correlations between the cumulative dose of dexamethasone and the first and second BSID-III scores.
3. Data collection and definition
Gestational age, sex, multiple gestations, birth weight, head circumference, delivery mode, 1- and 5-minute Apgar scores, and prenatal steroid use were examined as perinatal factors potentially affecting developmental delay. Maternal age, hypertension, and gestational diabetes were also examined. In terms of morbidities of the enrolled preterm infants in the NICU, we examined respiratory distress syndrome, BPD, postnatal steroid use, and retinopathy of prematurity (ROP), for which an intravitreal injection of bevacizumab or laser therapy was performed; patent ductus arteriosus, for which pharmacotherapy or ligation was performed; necrotizing enterocolitis for which a laparotomy was performed; inguinal hernia surgery; culture-proven sepsis; referred otoacoustic emission or auditory brainstem response; and weight and head circumferences at the time of discharge [8]. The presence and severity of BPD were determined on the basis of the need for oxygen therapy 28 days after birth and at the corrected age of 36 weeks. BPD was considered mild when the infant required oxygen therapy at 28 days after birth but no longer required oxygen therapy after the corrected age of 36 weeks; moderate when the infant required <30% oxygen administration; and severe when the infant required ≥30% oxygen administration or positive-pressure ventilation [9].
Postnatal steroids were used for two main reasons in the NICU. Hydrocortisone was administered at 3 mg/kg/day for refractory hypotension not treated by dopamine administered at ≥10 µg/kg/min. The dose of hydrocortisone was gradually reduced, and administration was stopped once the blood pressure stabilized. Dexamethasone was administered from at least 3 weeks of age when the infant was exposed to oxygen therapy or positivepressure ventilation for a long period after being diagnosed with BPD or when progression to severe BPD was predicted and weaning from invasive mechanical ventilation was deemed difficult even before 28 days after birth. Two administration schemes were used and selected by neonatologists based on the patient’s lung condition and the need for respiratory assistance: 10-day administration (with an initial dose of 0.1 mg/kg/day gradually reduced over 10 days or a total dose of 0.55 mg/kg) or 2-week administration (with an initial dose of 0.25 mg/kg/day gradually reduced over 14 days or a total of 1.62 mg/kg). When the infants could not be weaned off mechanical ventilation even after 3 to 4 days of dexamethasone administration, steroid administration was deemed ineffective and was ceased. When weaning from mechanical ventilation was delayed, steroids were administered at regular intervals.
4. Statistical analysis
All analyses were performed using R version 3.6.1 (R Core Team 2017, R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/). The clinical characteristics of the study population were described as means±standard deviations or numbers (percentages) of cases. Univariate and multivariate logistic regression models were used to identify the risk factors for developmental delay, and associations were presented as odds ratio (OR) and 95% confidence interval (CI). Pearson correlation analysis was performed to analyze the relationship between the total accumulated dose of dexamethasone and the composite score for the development domain. Furthermore, a simple linear regression model was fitted for the BSID-III test scores within and by each development domain after the corrected age of 24 months. Statistical significance was set at P<0.05.
RESULTS
1. Study population
A total of 254 VLBWIs weighing <1,500 g were admitted to the NICU of our institution between January 2014 and December 2020. Of these, 149 infants who did not complete the BSID-III test, 1 infant who completed the Korean Denver Development Screening Test II, and 2 infants who completed the BSID-III at times other than during the specified period were excluded. The remaining 102 infants completed their first BSID-III test at the corrected ages of 12 to 24 months. Thirty-one infants with severe brain lesions (six with IVH grade III or higher, 21 with PVL, and four with IVH grade III or higher with PVL) were excluded. Finally, 71 infants were included in this study (Figure 1). The mean gestational age and birth weight of the included infants were 29.3±2.6 weeks and 1,087.5±252.4 g, respectively (Tables 1, 2). Thirty-six infants completed the second BSID-III test after the corrected age of 24 months (mean corrected age, 28.2±6.5).
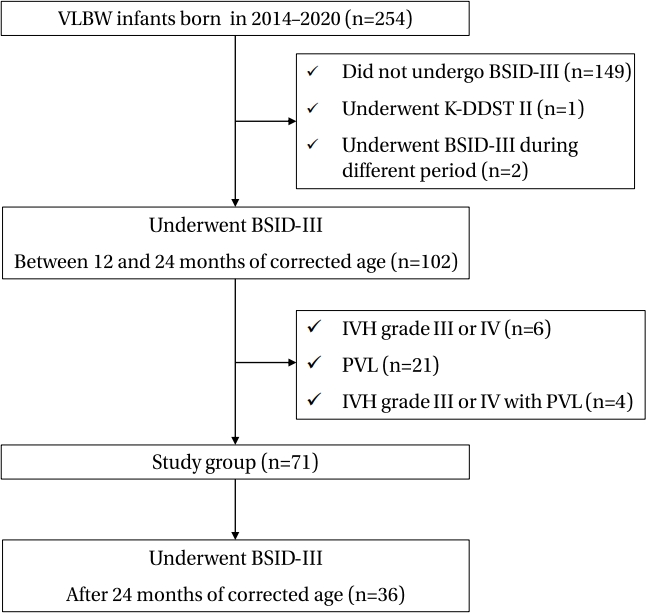
Enrollment of the study group. Abbreviations: VLBW, very low birth weight; BSID, Bayley Scales of Infant and Toddler Development; K-DDST, Korean Denver Developmental Screening Test; IVH, intraventricular hemorrhage; PVL, periventricular leukomalacia.
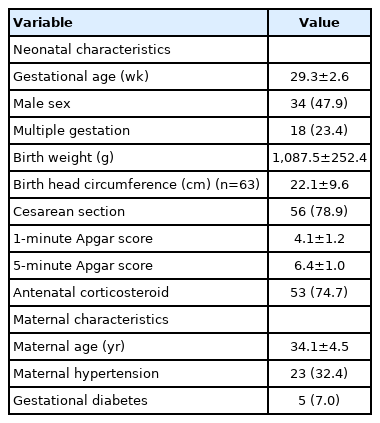
Demographic Characteristics of the Enrolled Preterm Infants (n=71)

Morbidities of the Enrolled Preterm Infant in the Neonatal Intensive Care Unit (n=71)
2. Neurodevelopmental assessment results
Seventy-one infants without severe brain lesions who completed the BSID-III test completed their first test at the mean corrected age of 14.7±3.3 months. Developmental delay was most commonly observed in the language domain (n=19, 26.8%), followed by the cognition (n=17, 23.9%) and motor domains (n=13, 18.3%). However, in the comparison of the mean composite scores and the percentage of infants with severe developmental delay among the domains, the motor domain had the lowest mean composite score (70.9±7.0) and involved the highest number of infants with severe developmental delay (n=6, 8.5%) (A in Table 3).

Overview of the Bayley Scales of Infant and Toddler Development Test Outcome of the Enrolled Infants
Of the 71 infants analyzed, 36 completed the second BSID-III test at a mean corrected age of 28.2±6.5 months. Developmental delay was most commonly observed in the language domain (n=17, 47.2%). The language domain had the lowest mean composite score (68.9±9.7) and involved the highest percentage of infants with severe developmental delay (n=7, 19.4%) (B in Table 3).
3. Predictors of adverse neurodevelopmental outcome
The risk factors for developmental delay were analyzed for each BSID-III domain. In the multivariate logistic regression analysis, mild BPD was identified as a risk factor of cognitive developmental delay (OR, 13.21; 95% CI, 1.75 to 139.35; P=0.02) between the corrected ages of 12 and 24 months, whereas prenatal steroid administration was found to reduce the risk of cognitive developmental delay (OR, 0.19; 95% CI, 0.03 to 0.84; P=0.04) (Table 4). In the univariate analysis, prenatal steroid administration was found to reduce the risk of language developmental delay (OR, 0.38; 95% CI, 0.14 to 0.95; P=0.05), and ROP was identified as a risk factor for motor developmental delay (OR, 6.00; 95% CI, 1.23 to 29.96; P=0.02). However, no significant risk factors were identified in the multivariate logistic regression analysis for either domain. The univariate and multivariate logistic regression analyses revealed no significant risk factors for cognitive or motor developmental delay after the corrected age of 2 years. Severe BPD was identified as a risk factor for language developmental delay (OR, 6.75; 95% CI, 1.38 to 50.81; P=0.03) only in univariate analysis. Postnatal dexamethasone use had no significant effect on the development delay for each domain in the univariate and multivariate logistic regression analyses at the corrected ages of 1 and 2 years.
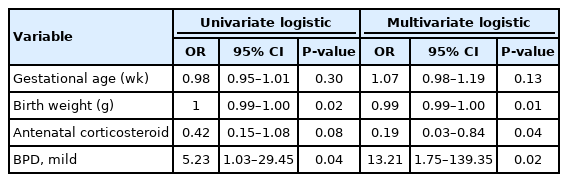
Univariate and Multivariate Logistic Regression for Cognitive Outcomes of Preterm Infants between the Corrected Ages of 12 and 24 Months (n=71)
4. Developmental changes at a corrected age of 1 and 2 years
Thirty-six infants completed the two BSID-III tests. The trends in developmental delay were analyzed by comparing the first and second BSID-III tests. The infants scored lower in the second test than in the first test across all domains, indicating developmental delay (Figure 2).
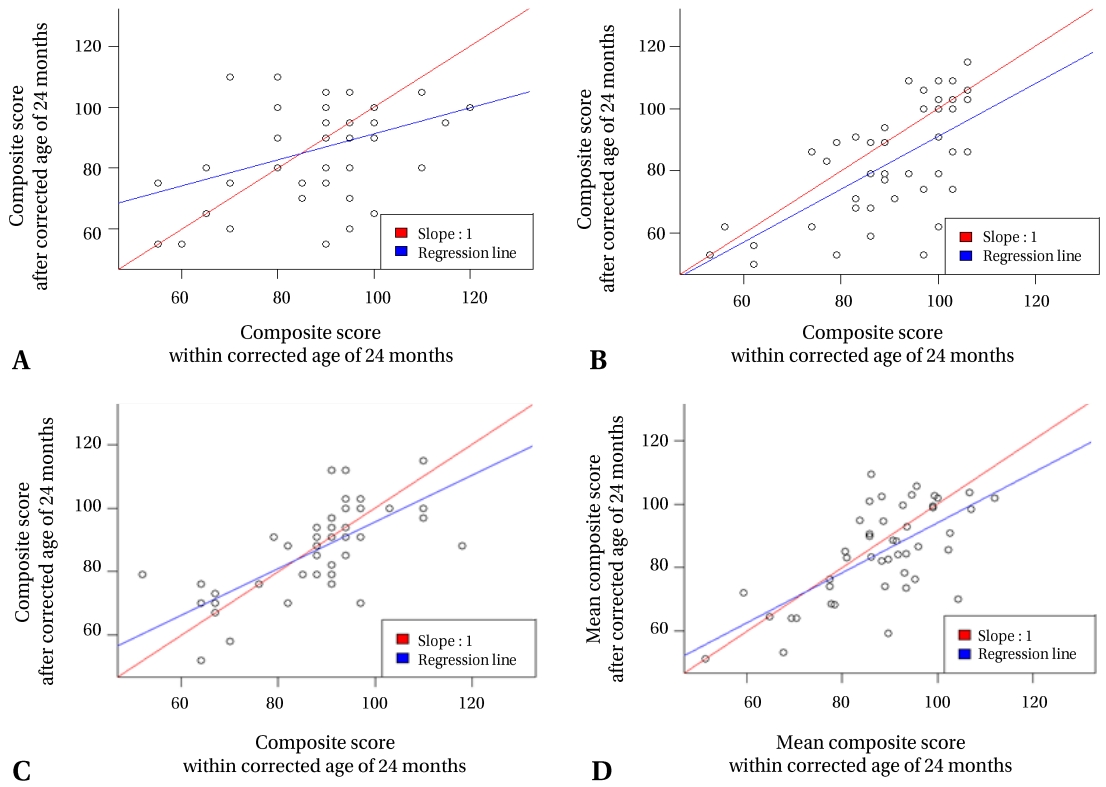
Simple linear regression for the results of the Bayley Scales of Infants and Toddler Development within and after 'the' corrected 'age' of 24 months according to the development domain. (A) Cognition domain, (B) language domain, (C) motor domain, (D) mean composite score of three domains.
5. Effects of dexamethasone use on the developmental assessment results
Of the 71 infants who completed the first BSID-III test, 37 were administered dexamethasone. The time of the first administration was 48.8±19.6 days (range, 23 to 111) after birth, and the total duration of administration was 21.4±14.3 days (range, 3 to 75). The cumulative dose of dexamethasone used was 3.8±3.7 mg/kg (range, 0.5 to 21.0).
Among the infants who completed the second BSID-III test, 23 had a history of dexamethasone use. The first administration was performed 48.5±19.7 days (range, 27 to 111) after birth, and the total duration of administration was 19.1±12.3 days (range, 3 to 50). The cumulative dose of dexamethasone was 2.8±1.9 mg/kg (range, 0.5 to 7.0).
No significant correlation was observed between the cumulative dose of dexamethasone and developmental delay based on the first BSID-III test scores; meanwhile, the second BSIDIII scores for the cognition (P=0.03) and language domains (P=0.02) were significantly decreased as the cumulative dose of dexamethasone increased (Figure 3).
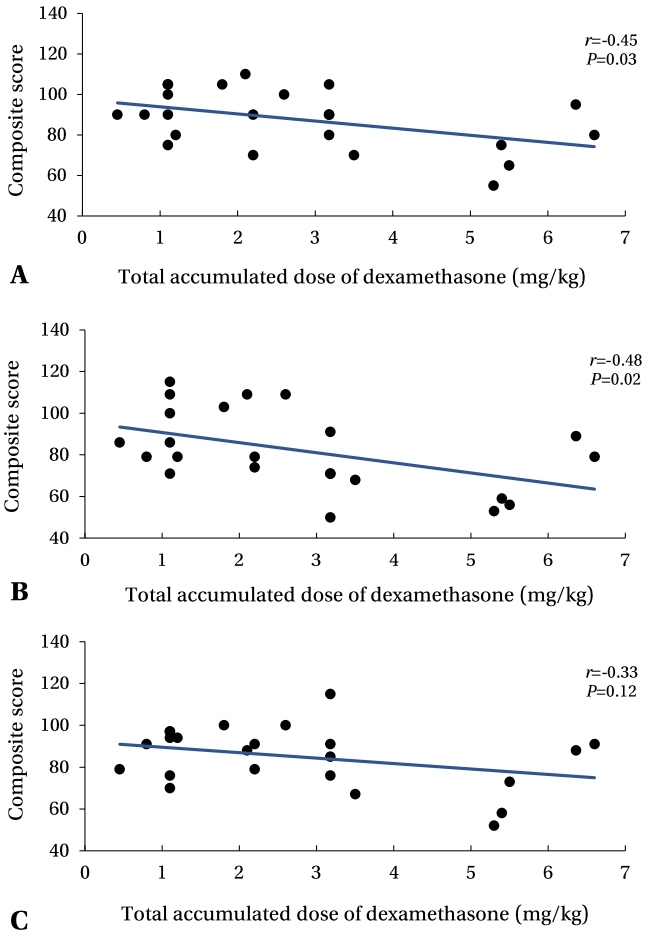
Scatter plots and Pearson correlation coefficients (r) between the total accumulated dose of dexamethasone and composite score by development domains after the corrected age of 24 months. (A) Cognition domain, (B) language domain, (C) motor domain.
DISCUSSION
Compared with full-term infants, preterm infants have underdeveloped executive functions, reduced receptive and expressive vocabularies, and poor motor function. The later a developmental delay is managed, the more likely it is that a preterm infant will experience cognitive, language, and motor disabilities that can require additional treatment. Therefore, early developmental assessment of preterm infants is important [10,11]. However, of the 254 VLBWIs treated in the NICU from 2014 to 2020 in this retrospective study, only 102 (40.2%) and 36 (14.2%) completed the BSID-III tests at the corrected ages of 1 and 2 years, respectively. The KNN, started in 2013, is a web-based VLBWI registration project with 75 participating hospitals, which currently includes approximately 70% of all VLBWIs registered across Korea [12]. Data from the KNN showed a poor developmental follow-up rate for preterm infants in South Korea. Only 28.7% and 11.9% of all VLBWIs completed a short-term developmental assessment between the corrected ages of 18 and 24 months in 2014 and a long-term assessment between the ages of 33 and 38 months in 2013, respectively [13]. Since the launch of the KNN and the strong encouragement of hospital participation, the incidence of short- and long-term developmental assessments has increased to 40.8% and 17.5%, respectively, for infants born in 2018 [14]. Although VLBWIs are a high-risk group for developmental delay, irrespective of the presence of brain disease, the follow-up rate for VLBWIs remains low at our institution and across Korea. Mothers who give birth prematurely are mostly concerned about the survival of their infants and their post-survival development. They feel hopeful that their infants show no abnormalities on brain imaging. During hospitalization, neonatologists must help parents recognize the necessity of developmental assessments by emphasizing the importance of long-term follow-up on neurodevelopment.
In this study, the incidence of language developmental delay was 26.8% and 47.2% at the corrected ages of 1 and 2 years, respectively. Language developmental delay is the most common and long-lasting developmental delay. This result is consistent with a report by the KNN, which stated that language developmental delay had the highest incidence of 26.5% to 48.7% among other types of delays [13-17]. Similarly, a study examining infants born without severe brain lesions between 2013 and 2015 reported that language developmental delay had the highest incidence (20.7%), and severe language developmental delay also had a high incidence (4.2%) [18]. Prior studies have reported that infants with a clear language developmental delay without neurological deficits continue to show language developmental delay until they reach school age [19]. Normal brain structure, articulators, and sensory-motor system are prerequisites for normal language development. Moreover, exposure to social stimuli and normal cognitive function are required to use language to communicate. Problems with any of these factors can lead to a language developmental delay, which may later be accompanied by behavioral disorders, such as attention deficit hyperactivity disorder and autism spectrum disorder, as well as learning disabilities. Structural assessment of the brain alone does not determine whether an infant will undergo normal language development. Language development must be regularly assessed because language developmental delay may be an early sign of other neurodevelopmental disabilities.
Low gestational age, low birth weight, low Apgar score, BPD, ROP, IVH, and PVL are known risk factors for developmental delays. Conversely, several studies have reported that prenatal steroid use reduce the risk of developmental delay [11,20-24]. In our study, prenatal steroid use contributed to normal development. However, in the multivariate analysis of the risk factors for developmental delay, mild BPD was identified as a significant risk factor for cognitive developmental delay at the corrected age of 1 year. This result is inconsistent with those of previous studies that have identified severe BPD as a risk factor for developmental delay [4,25]. This discrepancy in the results may be attributed to the small sample size used in our study or to a bias caused by factors not considered herein. Thus, it cannot be concluded that mild BPD is a better predictor of poor neurodevelopment than moderate-to-severe BPD.
Dexamethasone exerts adverse effects on neurodevelopment and is more dangerous the earlier it is used [26,27]. Davidovitch et al. [28] reported that 113 (2.3%) of 4,963 VLBWIs were diagnosed with autism spectrum disorder, suggesting a significant association between postnatal steroid use and autism spectrum disorder. Conversely, a recent meta-regression study reported that infants at a higher risk of developing BPD had increased rates of survival free of CP after postnatal corticosteroid therapy [29], suggesting the possibility of using minimal doses of postnatal steroids if weaning from mechanical ventilation is difficult [30]. This study investigated whether dexamethasone use affects the development of preterm infants at our institution. Although the cumulative dose of dexamethasone did not affect development at the corrected age of 1 year based on the first BSID-III test, it was significantly correlated with low second BSID-III scores at the corrected age of 2 years. The long-term adverse effects of dexamethasone use might have contributed to the lower second BSID-III scores of the 36 infants who completed the two BSID-III tests at 1-year intervals. However, history of drug administration is not the only factor that affects development. Environmental factors, such as post-discharge parental nurture and nutrition, can also have a large effect. Considering the small sample size of this study, it cannot be concluded that the long-term adverse effects of dexamethasone cause developmental delay. A largescale, well-designed, prospective study with a long-term follow-up is needed to address this issue.
In this study, some infants without severe brain lesions, who were not administered dexamethasone, showed developmental delay. Among them, five patients showed diffuse excessive high signal intensity (DEHSI). While prior studies have reported a correlation between severe white matter damage and neurodevelopmental delay, more recent studies have reported no such correlation [31-37]. Therefore, this study did not include DEHSI as a severe brain lesion. Twenty-four patients in our study showed DEHSI; however, 76% of these patients (n=19) showed normal development, suggesting that DEHSI may not be considered a severe brain lesion. Our results showed that developmental delay occurs in VLBWIs lacking severe brain injuries and postnatal dexamethasone administration. Without follow-up developmental assessments, a caregiver may notice the delay only after it has already progressed significantly and the optimal timing for rehabilitative therapy has been missed. Therefore, a follow-up assessment to determine whether development occurs at an expected rate is necessary for early screening and treatment.
This study has several limitations. This study had a small sample size given that it was a single-center study, and the incidence of BSID-III test administration was low (40%) among the participating infants. Additionally, as this was a retrospective study, the time at which the BSID-III test was administered varied among the infants and the history of rehabilitative therapy before the developmental assessments was not considered. Finally, hydrocortisone use was not considered, even though some infants had a history of hydrocortisone administration; therefore, the total effect of steroid uses could not be assessed.
However, because this study was conducted at a single institution, it was possible to assess the developmental state of VLBWIs discharged without severe brain lesions after they receiving uniform care under the same guidelines. This study differed from previous studies that have reported severe brain injuries as a major risk factor for developmental delay, as it assessed the risk factors for developmental delay in preterm infants without severe brain lesions. Additionally, this study monitored improvements in or worsening of developmental delay during the follow-up appointments. In NICUs, it is common to observe parents obsess over the brain MRI results of their preterm infants during hospitalization. If no severe brain lesions are detected, parents tend to ignore the doctor’s recommendation to pursue followup developmental assessment. This study demonstrated that preterm infants without severe brain lesions can still experience developmental delay that may persist as age. This finding may help healthcare professionals and parents of preterm infants recognize the importance of developmental follow-up. A multidisciplinary effort from healthcare professionals is needed to ensure systematic, long-term follow-up and management, in addition to a large-scale prospective study examining the positive effects of such efforts on the development of VLBWIs.
Notes
Ethical statement
This study was approved by the Institutional Review Board of the Pusan National University Hospital (IRB No. 05-2021-297). The requirement for informed consent was waived by the board.
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
Author contributions
Conception or design: M.H.J., Y.M.H.
Acquisition, analysis, or interpretation of data: M.H.J., S.H.J., S.J.P., N.L., M.H.B., K.H.P., S.Y.B., C.K., Y.M.H.
Drafting the work or revising: M.H.J., Y.M.H.
Final approval of the manuscript: All authors read and approved the final manuscript.
Funding
None
Acknowledgements
None